Subacute Sclerosing Panencephalitis
Introduction
Subacute sclerosing panencephalitis (SSPE) is a rare disease of the brain which results in progressive loss of physical and mental skills.
What is the cause?
SSPE is caused by an unusual response to the measles virus which reactivates in the brain, often many years after the original infection. The presence of the virus within the brain cells prevents them working properly and passing messages to each other. The brain is the control centre of the whole body so blockages in the messages to other parts of the body will prevent those parts working efficiently even though the parts themselves are quite healthy.
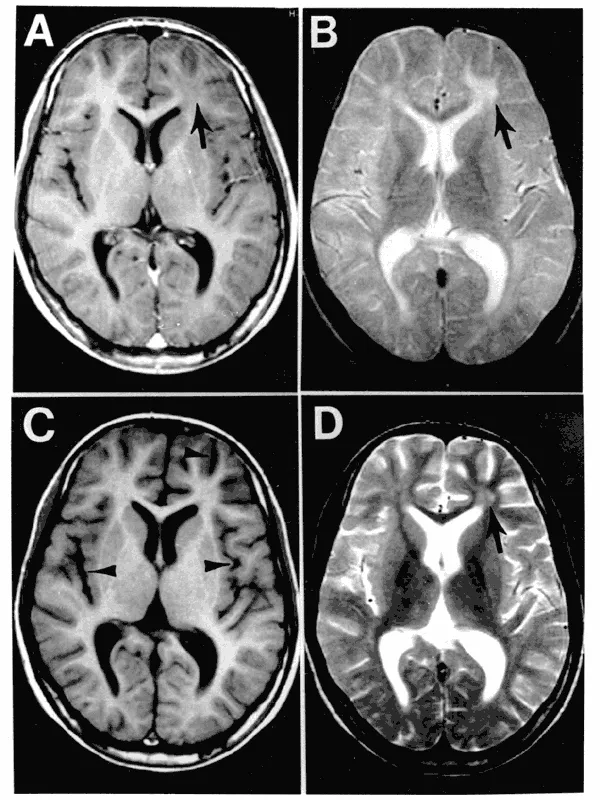
How is it diagnosed?
The diagnosis is usually suggested by an electroencephalogram (EEG) which shows particular brain wave patterns, and is confirmed by examining the cerebro spinal fluid(CSF) which shows the measles antibodies in the fluid surrounding the brain.
Does it have any alternative name?
SSPE was first described at the beginning of the 20th century and its descriptive name is the one by which it has been known since then.
Is it inherited?
SSPE is not inherited. It is not fully understood why one particular child should develop this late complication after a ‘normal’ attack of measles which may have affected other family members at the same time; other children in the family do NOT appear to be at any greater risk of developing the same complication.
How common is it?
It is estimated that the incidence in the UK is approximately 1: 1000,000; the incidence is lower in countries where the use of measles vaccine is more widely enforced.
How does the disease progress?
The child will usually start having some changes in behaviour and problems with learning or school work, and may have been seen by a psychologist or psychiatrist. The child develops involuntary movements which make him/her stagger or fall backwards, as if pulled by an invisible string. Deterioration in the thought processes continues and myoclonic jerks start affecting different parts of the body, coming on like a sudden shock and fading over a few seconds; these particular spasms are very typical and are experienced by all sufferers of SSPE; epileptic seizures may or may not occur. As the condition progresses the child/ young person becomes totally dependent on others for all their care ; eventually he/ she will fall into a coma. The rate of deterioration can vary very considerably and it is not usually possible to predict how long the course of the illness may be.
Eventually, however, the combination of the diseased brain and physical weakness becomes too great to sustain life. In some people the course of the illness can be very rapid, leading to death within 9 months of the onset of the symptoms whilst in others the course of the disease can be much slower, with periods of stability, over 10 – 15 years. The condition is not a painful one and the child/young person will mercifully be unaware of what is happening in the later stages of the disease. It is, however, cruelly distressing and frustrating for the child whilst he/ she is aware of the deterioration in abilities, and for the family and friends throughout the illness. Parents and carers will be aware of the child’s increasing frailty whilst he/ she is comatose, and death is relatively peaceful and expected when the time comes.
Is there any treatment?
As yet, there is no curative treatment; trials of various antiviral agents and drugs which affect the body’s response to infections have, sadly, not proved of any significant benefit so far. The extreme rarity of the condition and the variable rate of progress of symptoms in different people makes assessment of responses to different drugs a slow process, with long term trials lasting several years. Every effort, however, is made to treat the symptoms; thus drugs can be given to help control seizures and jerks/spasms and other problems as they occur; pain relief and sedative drugs can be given if required and feeding can be assisted. Physiotherapists and others can advise parents on positioning, seating and exercising the limbs to maintain comfort. Specialist schooling will be required and it is important for the child/ young person to have this stimulating environment and social contact and, indeed, for the parents to have some time for themselves and other family members and friends. Though not scientifically proven, many children gain some symptomatic relief from some forms of complementary therapies such as cranial osteopathy and massage etc.
Is any research being done?
Research is on-going into trying to understand the mechanism of this tragic disease, why the common measles virus very rarely has this devastating effect on some people, and into potential treatments. Sadly, no effective treatment has yet been found and any discoveries in the future would be likely only to be able to slow or halt the progression rather than repair damage already sustained. Your neurologist will keep you informed of any research and drug trials being conducted.
Is there a Support Group?
The Encephalitis Society can provide written information, telephone advice, support and contact ( if wanted) with other families:-
Encephalitis Society
Encephalitis Resource Centre
7b Saville Street
Malton YO17 7LL
Tel / Fax : 01653 699599
e-mail : [email protected]
C.Mostyn GOSH 2005
Web : http://www.encephalitis.info